
baobab soluciones presents a tool to improve efficiency and reduce waiting lists in the surgical block with the collaboration of the Ramón y Cajal University Hospital.

Data from the World Health Organization show that the rate of aging of the world’s population has grown much faster than in past decades. We demand a greater amount of health services and consequently, there is a greater probability of requiring one or more surgical interventions throughout our lives.
At this point, the countries face the important challenge of guaranteeing that their health systems accept this demographic change and use surgical waiting lists as a key indicator to measure their quality and efficiency.
In 2020, baobab soluciones highlighted the advantages of Artificial Intelligence and Prescriptive Analytics for intervention programming compared to the industry standard, in which a person manually assigns operations and resources to operating rooms. A management system for surgical operations and resources based on these techniques would provide a substantial improvement in average waiting times and would intelligently support managers’ decision-making, making it possible to automate this task under medical supervision when the time comes.
What a couple of years ago was presented as an idea, baobab solutions has turned into a real tool thanks to a grant awarded by Red.es at the end of 2021 to promote the experimental development of solutions, applications or services that, among other things, improve the efficiency of health services; and the collaboration of the Ramón y Cajal University Hospital in the tasks of taking specifications and validating the tool.
How are operating rooms currently programmed?
The programming of operating rooms is carried out similarly in various hospitals in the national territory, although we can find some variations between them.
1.- Operating rooms are assigned to surgical services.
2.- Each surgical service schedules its interventions on a weekly basis apart from the rest of the hospital services and sends their schedules to the Central Medical Committee.
3.- The Central Medical Committee is in charge of finding and resolving incompatibilities such as the lack of medical personnel due to sick days or vacations, the lack of ICU beds…
This way of working allows the Committee to start from an initial solution that is not the best possible and as a consequence a high number of changes must be evaluated manually. As a result it will be difficult to find an optimal schedule of interventions in terms of productivity and efficiency, which has a negative impact on waiting lists.
Why baobab?
In an inefficient context, which poses a highly complex problem with numerous variables and in the absence of tools on the market specially designed for resource management and task sequencing in the surgical suite, Advanced Analytics allows automating the programming of surgical interventions as well as the health resources (human and material) necessary to carry them out. At baobab we are specialists in custom optimization solutions that enhance decision-making using techniques such as Prescriptive Analytics, Artificial Intelligence or Digital Twins. We consider this problem to be a perfect fit for us and we consider ourselves very lucky to have the trust of Red.es to develop the solution.
Let’s review the complexity of the problem
We needed to create a tool that would work with a series of data:
- Information on surgical services, surgical units into which the surgical services are divided, procedures performed and their standard duration.
- Information about patients: surgical department, unit and surgeon who put them on the waiting list, date of entry on the waiting list, medical priority, procedures they need, etc.
- Information on operating rooms: availability, assignment to surgical services, units and surgeons, and the existence of special characteristics that mean that certain interventions must be performed in one operating room or another.
- Information on surgeons, anesthetists and nurses: surgical departments and units to which they belong or in which they can work, availability, specialization (if applicable) in a specific procedure and number of medical resources needed per procedure.
- Information on material resources needed by procedure (laparoscopy devices, ICU beds, etc.) and their availability.
- Information about support teams for interventions, such as cleaning teams or warders.
- Information on sources of variability: delays in the start of the first intervention of a day/shift and in the duration of the interventions.
- Maximum occupancy of operating rooms by surgical service that is not to be exceeded before incorporating the uncertainty that exists in the system.
With these elements, the tool should provide the following:
- Information on the patients attended per day and operating room.
- Medical resources assigned to each intervention (surgeons, anesthetists and nurses).
- Material resources necessary during and after each intervention (laparoscopy devices, ICU beds, etc.).
- Transportation needs by the attendants for each patient.
- Cleaning needs of the operating rooms after each intervention.
- Patients whose maximum waiting time has been exceeded before being operated on.
- Occupancy of the operating rooms.
Percentage of operations that end without incident (delays or cancellations) after introducing the uncertainty that exists in the system and coefficient of variation for this measure.
What is the flow of use for the tool?
On a baseline scenario, the tool proposes a schedule of operating rooms that complies with the hospital’s allocation rules, that does not exceed the maximum occupancy percentage defined by each surgical service for its operating rooms, and that does not present conflicts in relation to the resources (human and material) necessary to carry out the interventions.
Starting from this solution, the tool also allows to:
1.- Analyze the percentage of operations that are expected to end without incident (delays or cancellations) by taking into account the uncertainty that exists in the system (delays in the start of operations, variability in the duration of operations…).
2.- Look for alternative solutions to the initial one, breaking any of the rules with which the hospital is currently working.
3.- Evaluate “what if” type changes on the starting solution with the purpose of iteratively optimizing the surgical unit. For example, by first analyzing what would happen if an underused operating room was assigned to a service unit or surgeon with a large waiting list and then analyzing what would happen if medical staff and operating rooms were provided in extraordinary slots to the service unit or surgeon that presented a longer waiting list.
In short, this tool can be used as a platform to test different surgical block management alternatives before putting them into practice in a real system.
Is it easy to work with such a tool?
Working with the tool is very simple thanks to its interface. For example, Figure 1 shows the screen that has been created to work with the input data, while Figure 2 shows a Gantt chart with the results of an operating room schedule that can be clicked on to obtain detailed information about each intervention.
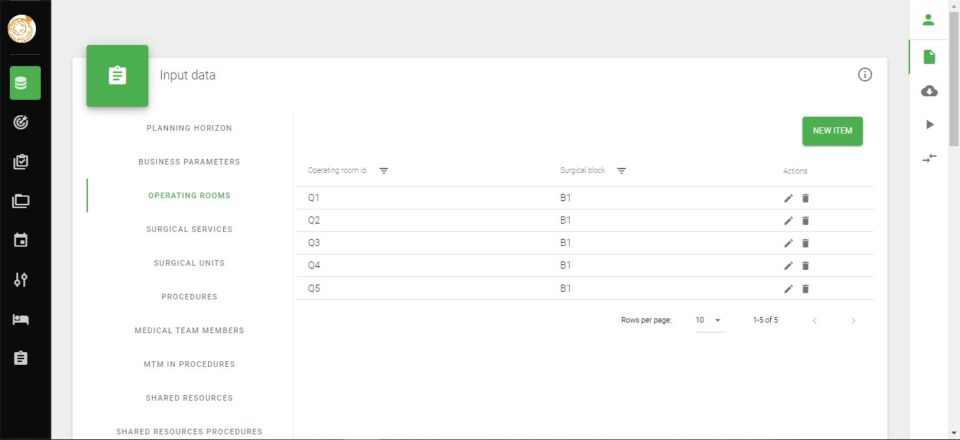
Figure 1. Example of input data screen.
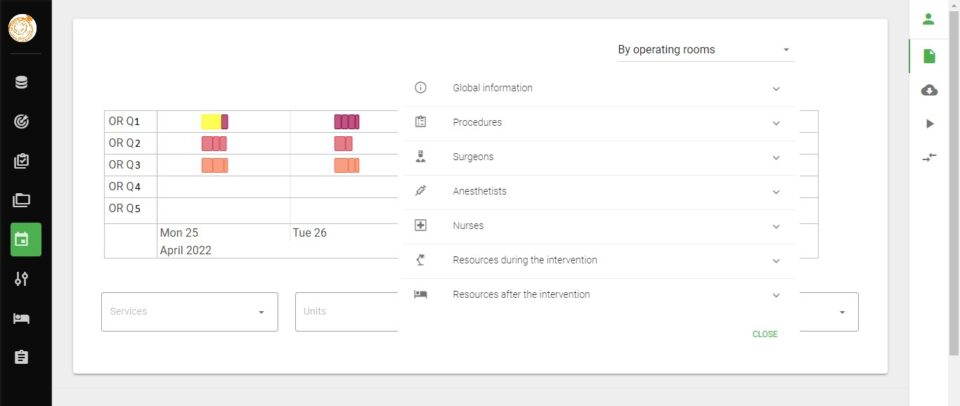
Figure 2. Example of output graph.
What results has the tool provided in a real environment?
The tool has been tested using partial data from a surgical service at Hospital Ramón y Cajal, composed of 4 units that work with a waiting list of 466 patients and have 17 slots (or combinations of operating room, day, shift and surgeon) for performing operations. In addition, in this case, a certain shared material resource (of which only one unit is available) is needed for the development of some interventions.
For this problem, an initial operating room schedule has been calculated in 2 minutes, the initial solution has been considered by the hospital as a good starting point on which to work and some of the improvement proposals made on this solution have aroused interest of the medical team for the tool, which demonstrates its potential.
baobab soluciones has a demo of the tool for those people in the health field who want to know its potential in more detail, as well as its ability to integrate with the systems of their own hospitals.